
Three stories - one plot


This picture taken around 1800 shows a very famous sight in Vienna known as ‘Naschmarkt’. Even today, at Naschmarkt you will find hundreds of people making their way through the stands, buying fruit, vegetables, meat, fish or sweets. What does this market have to do with echo? Read on and find out.
Three stories - one plot
We wrote a little play for you. A play based on true facts and actual people, which takes place at or around Naschmarkt in Vienna.Let me first introduce our main characters:
Act one, Scene one: Victor
Victor is a 71-year-old tourist in Vienna. He walks through the crowded lanes of Naschmarkt, where he suddenly collapses in front of his wife who immediately calls the EMS.When the EMS arrives Victor is disoriented, breathing spontaneously, and hypertensive. His ECG shows sinus tachycardia. The paramedics apply antihypertensive medication and bring him to our ED.
Act one, Scene two: Sandra
Our main female character, Sandra, is 29 years old and not far from Naschmarkt. She is at her GP's private practice which is just a block away from where Victor collapsed. She has been experiencing breathing difficulties for 6 days. Her doctor establishes an oxygen saturation level of 89% and calls the EMS. He suspects severe pneumonia.
Act one, Scene three: Gerald
Just down the street, Gerald is at home with back pain, fever and shortness of breath. He is 56 years old and has no relevant medical history. The symptoms started just a couple of minutes ago, but now he is too weak to even walk to the bathroom. He calls a friend to bring him to the hospital (we think it would have been better if he had called the EMS!). Three characters, three different lead symptoms: collapse, dyspnea and fever with back pain. What do these three have in common?
Act two, Scene one:
The second act takes place at our emergency department - which is where they all come together. Luckily Gerald (who was taken to the hospital by his friend) also reached the ED alive. We performed an ECG in all three patients. This is what we found:
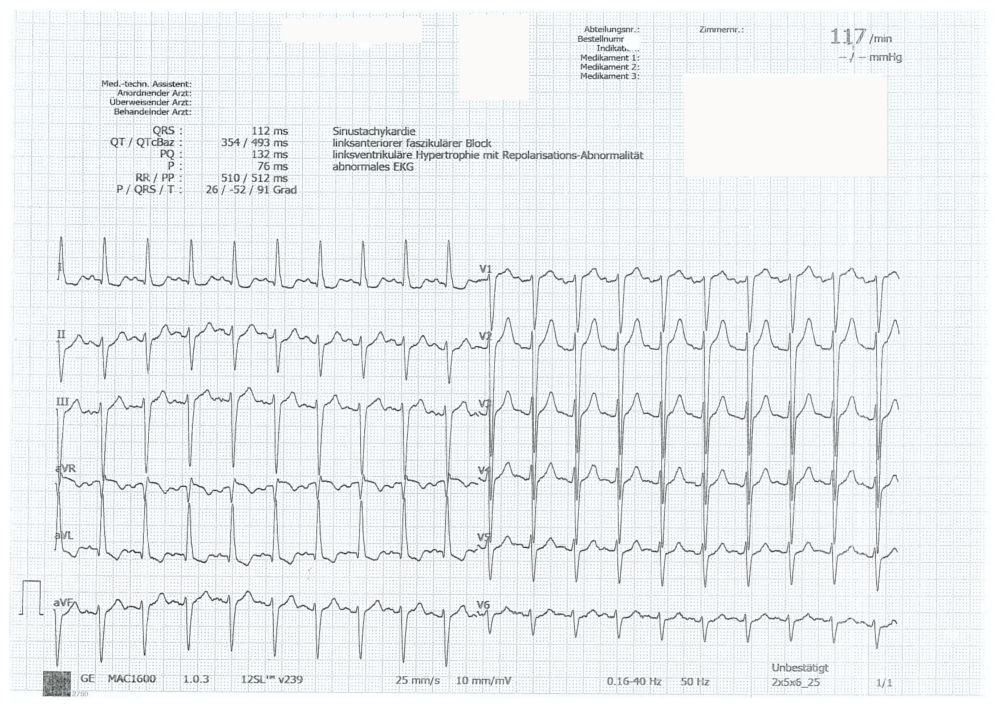
Patient 1 - Victor
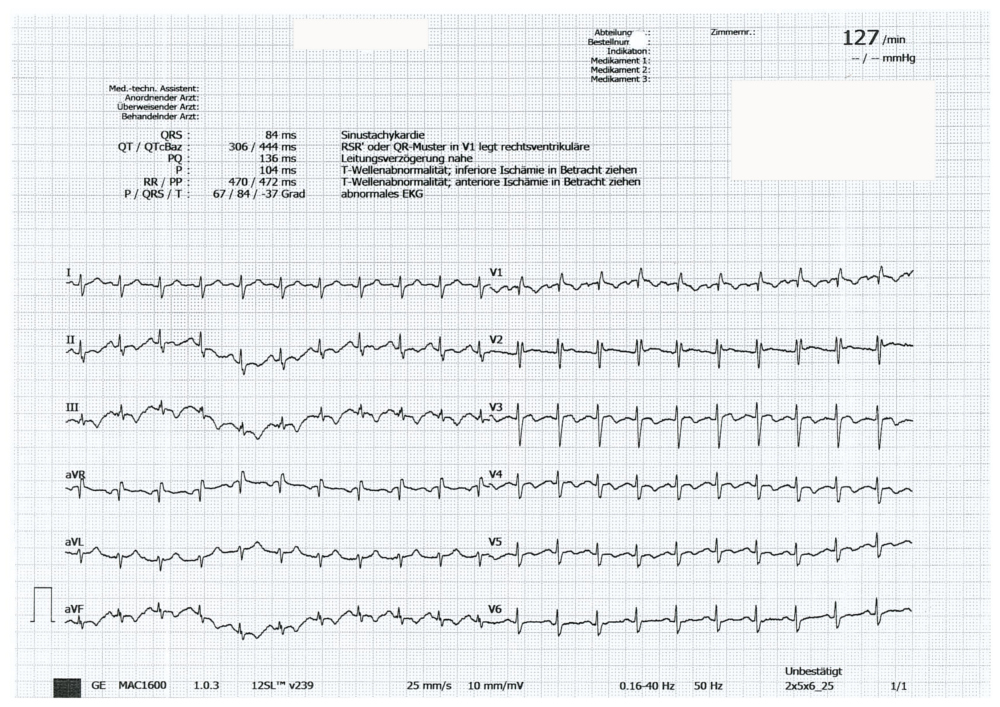
Patient 2 - Sandra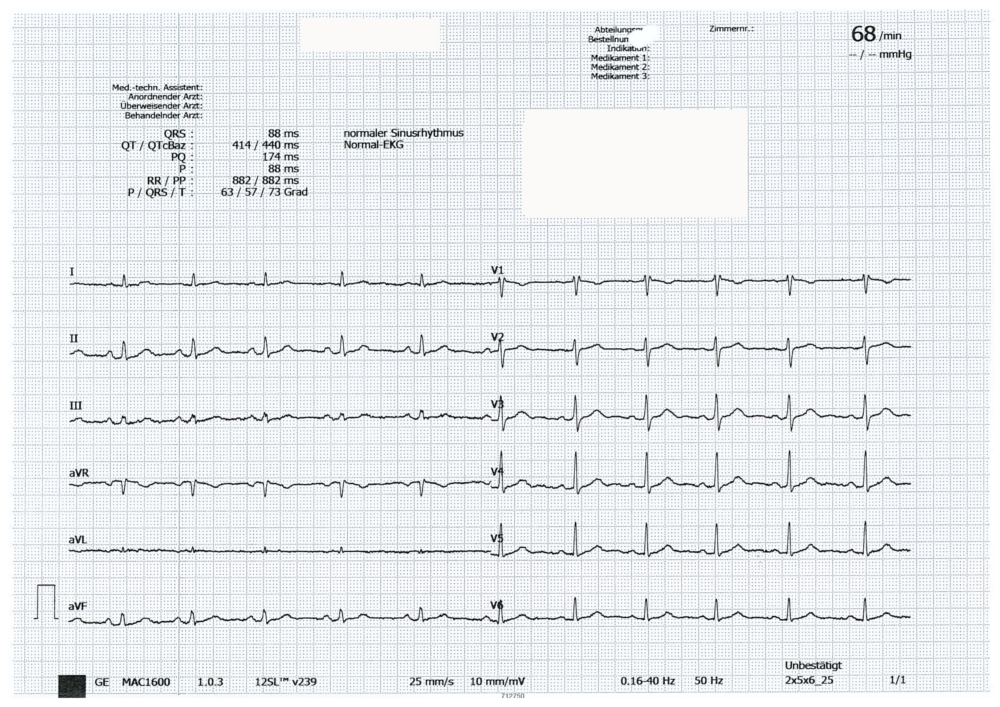
Patient 3 - Gerald
While waiting for the lab results we had time to perform echocardiography. Look what we found:
Video Platform Video Management Video Solutions Video Player
Short-axis view of Victor: compare the size of the right
ventricle with that of the left ventricle.
Video Platform Video Management Video Solutions Video Player
Short-axis view of Sandra: look at the motion of the
interventricular septum
Video Platform Video Management Video Solutions Video Player
Short-axis view of Gerald: very small hyperdynamic left
ventricle. Is anything else abnormal?
What do these three patients have in common? All three have right ventricular enlargement and dysfunction, and all three have evidence of right heart pressure load. Maybe there is a common cause. Here you have some CT images that possibly confirm what you have already suspected:


This is Victor'CCT scan – note the central
thromboembolism in the left and right pulmonary artery.


Sandra also had a bilateral pulmonary embolism.
Note the rather significant degree of
obstruction.


Gerald’s CT shows a very similar condition - bilateral
pulmonary embolism.
A short “rehearsal”:
Pulmonary embolism (PE) is a common and often severe or even fatal manifestation of venous thromboembolic disease. It is caused by a thrombus obstructing the pulmonary artery or one its branches (much less frequently it might be a tumor, air, or fat). This condition is observed in about 100/100,000 persons, but is more frequent in hospitalized patients. PE is usually caused by venous thrombi of the lower extremities, which are shifted by the blood stream through the right heart into the pulmonary vessels. Severe acute PE may cause right heart failure and consecutive shock.
What the patients feel:
- dyspnea at rest or with exertion (sudden onset), and tachypnea
- pleuritic pain
- cough / hemoptysis
- calf or thigh pain and swelling, and other symptoms of deep vein thrombosis (DVT)
- tachycardia
Echocardiography is not very sensitive in detecting pulmonary embolism. Actually, only emboli affecting a large portion of the vascular bed can be detected with echo. However, in these patients will you find typical sings of right ventricular enlargement, “D-shaped ventricle, and the Mc Connell sign (hypokinesia of the mid free lateral wall with hyperdynamic function of the apex). Compare the echos in the three patients. Can you see which right ventricle is affected most? I would say Gerald's. He also appears to have the most severe embolism. Still, the degree of embolism does not always correlate with the severity of right heart dysfunction. Patients who have a conditioned right ventricle (i.e. chronic pulmonary hypertension) can cope with acute pressure loads more easily than those who have “untrained” right ventricles. And don’t forget: if tricuspid regurgitation is present the right ventricle might appear better than it actually is. Back to our play:
Act two, Scene two – the treatment
In addition to intravenous volume supplementation, we wanted to achieve rapid anticoagulation (as secondary prophylaxis) in all three patients. Gerald and Sandra were given low-molecular-weight heparin from the start. Victor was initially given unfractionated heparin because it was yet unclear whether he could be stabilized without systemic thrombolysis.Fortunately, he could be put on low-molecular-weight heparin the next day. All three could be transferred to our normal cardiology ward after one day at the emergency department ICU.
The great finale:
All three could be discharged in good clinical condition and all of them returned to their baseline cardiac function with full exercise capacity. Of course they had to take oral anticoagulants. So a happy end after all.
Addendum and final scene (fictional ending):
Sandra, Victor and Gerald are sitting happily at a pleasant café in “Naschmarkt”, drinking a glass of wine and celebrating their recovery.

PS: Can you spot what's wrong with this image? ;-) If so, post your answers in the comments section
PPS: If you want to become a true echo expert and detect pulmonary embolism faster than everyone else. Well, then you might want to register for our Masterclass. Spots are limited - so put your name on the waiting list today!
Related Courses

The Echo MasterClass is the most comprehensive premium online course in echocardiography,…