
Hypertrophic Pyloric Stenosis
Case Presentation
3-month-old child with explosive, non-bilious vomiting after breastfeeding. An upper abdominal ultrasound was requested.
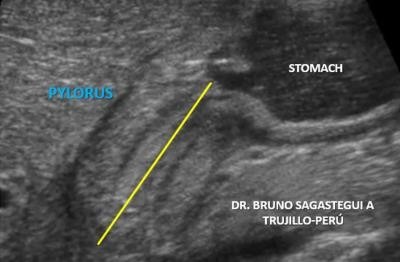 Caption: Longitudinal plane through right upper quadrant. | Description: Longitudinal plane showing the elongated pylorus with thickened pyloric muscle, “CERVIX SIGN”. We mean the channel length.
Caption: Longitudinal plane through right upper quadrant. | Description: Longitudinal plane showing the elongated pylorus with thickened pyloric muscle, “CERVIX SIGN”. We mean the channel length.
First published on SonoWorld
 Caption: Longitudinal plane through right upper quadrant. | Description: Longitudinal plane showing the elongated pylorus with thickened pyloric muscle, “CERVIX SIGN”. We mean the anteroposterior diameter and the thickness of the muscular layer.
Caption: Longitudinal plane through right upper quadrant. | Description: Longitudinal plane showing the elongated pylorus with thickened pyloric muscle, “CERVIX SIGN”. We mean the anteroposterior diameter and the thickness of the muscular layer.
 Caption: Transverse plane through right upper quadrant. | Description: Transverse plane showing “TARGET SIGN” with thickened pyloric muscle.
Caption: Transverse plane through right upper quadrant. | Description: Transverse plane showing “TARGET SIGN” with thickened pyloric muscle.
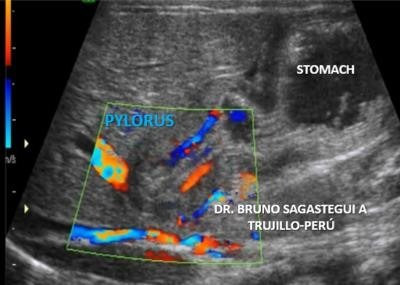 Caption: Longitudinal plane through right upper quadrant. | Description: Color Doppler examination of the pylorus showing vascularity in the mucosa and pyloric muscle.
Caption: Longitudinal plane through right upper quadrant. | Description: Color Doppler examination of the pylorus showing vascularity in the mucosa and pyloric muscle.
Differential Diagnosis
Pylorospasm
Gastro-oesophageal reflux
There is usually little differential when imaging findings are appropriate.
Of course, clinically it is important to consider other causes of vomiting in infancy.
A degree of pylorospasm is common in infancy and is responsible for some delay in gastric emptying. The pylorus, however, appears sonographically normal. In cases where the doubts persist, fluid gastric distention can be performed to "open" a tapered pylorus.Gastro-oesophageal reflux which represents the cause of vomiting in two-thirds of infants referred to radiology1.
Final Diagnosis
Pyloric hypertrophy
Discussion
Ultrasound is the modality of choice in the right clinical setting because of its advantages over a barium meal are that it directly visualises the pyloric muscle and does not use ionising radiation. Unfortunately, it is incapable of excluding other diagnoses such as midgut volvulus. Easy ultrasound technique is to find gallbladder then turn the probe obliquely sagittal to the body in an attempt to find pylorus longitudinally2. The hypertrophied muscle is hypoechoic, and the central mucosa is hyperechoic.
Diagnostic measurements include (mnemonic "number pi"):
- pyloric muscle thickness, i.e. diameter of a single muscular wall on a transverse image: >3 mm (most accurate3)
- length, i.e. longitudinal measurement: >15-17 mm.
- pyloric volume: >1.5 cc.
- pyloric transverse diameter: >13 mm
With the patient right side down the pylorus should be watched and should not be seen to open.
Described sonographic signs include:
- antral nipple.
- cervix sign
- target sign
Increased flow accompanies and may conceivably represent an integral component of the changes that occur with infantile hypertrofic pyloric stenosis4.
Follow Up
The baby was operated (pyloromyotomy) and did well
Technical Details
Ultrasound scanner. - Voluson 730 PRO. General Electric.
Transducer. - 10-12MHz linear array
Scanning in both transverse and longitudinal planes.
Case References1. Donnelly L, Jones B, O'hara S et-al. Diagnostic imaging. AMIRSYS. (2005) ISBN:141602333X. Read it at Google Books -
Find it at Amazon
2. Donnelly LF. Pediatric Imaging. Saunders. (2009) ISBN:1416059075. Read it at Google Books - Find it at Amazon
3. Blumhagen JD, Maclin L, Krauter D et-al. Sonographic diagnosis of hypertrophic pyloric stenosis. AJR Am J Roentgenol. 1988;150 (6): 1367-70. AJR Am J Roentgenol (abstract) - Pubmed citation
4. Hernanz-Schulman M, Yuwei Z et-al. Hypertrophic Pyloric Stenosis in Infants: US Evaluation of Vascularity of the Pyloric Canal. RSNA Radiology 2003, 229: 2. https://doi.org/10.1148/radiol.2292021303.