
2.5 Spectral Doppler
Spectral Doppler is an integral part of any exam. Both pulsed and continuous Doppler should be used. Which technique is applied depends on the blood flow velocity that you anticipate. PW displays velocities of approximately 1.7 to 2.5 m/sec (also see Chapter 1, Principles of Echocardiography). This section will address the views and settings in which spectral Doppler should be applied.
2.5.1 Spectral Doppler of the Right Ventricular Outflow Tract, Pulmonary Valve and Pulmonary Artery
Several views and windows can be used to record a Doppler signal of right ventricular outflow velocity. The most commonly used view is the parasternal short axis view, which is optimized for RV outflow (see PSAX base view as well). However, in many instances other views provide superior results. Especially the subcostal short-axis view provides spectral tracings of good quality. Placement of the sample volume and the mode of spectral Doppler one uses (CW vs. PW Doppler) depend on the pathology and the entity one is looking for. Use CW Doppler in the setting of pulmonary stenosis or RVOT obstruction. PW Doppler is generally better to obtain tracings that permit assessment of timing intervals such as pulmonary acceleration time (see Chapter 16, Right Heart Disease). Here the Doppler sample volume should be placed "within" the pulmonary valve. You will record a negative spectrum (below the zero line).
2.5.2 PW Doppler of Mitral Inflow
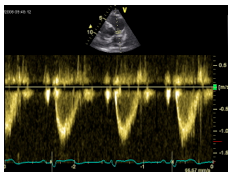
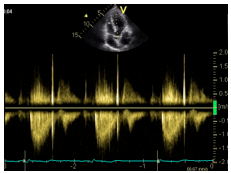
To record the mitral inflow signal use an apical four-chamber view (or an apical long-axis view). The Doppler sample volume is placed between the anterior and the posterior leaflet. Make sure that the sample volume is at the tip of the leaflets and you are parallel to mitral inflow. Color Doppler is useful to visualize the exact position and direction of mitral inflow.
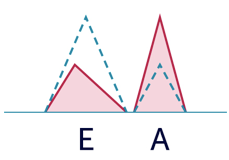
A very sharp initial signal occurs when the sample volume interferes with the mitral valve leaflets.In the presence of sinus rhythm you will see an "M-shaped" inflow pattern. The first wave is the "E" wave (early filling) while the second is known as an "A" wave (atrial contraction). The mitral inflow signal provides valuable information on diastolic function and left ventricular filling pressures. You can also measure time intervals of diastole (diastolic filling time, E-wave deceleration time, etc.). Spectral Doppler of mitral inflow is used to quantify mitral stenosis. However, as velocities in mitral stenosis frequently exceed 2 m/sec, one frequently needs CW Doppler in this setting.
2.5.3 PW Doppler of Left Ventricular Outflow Tract Velocity
This tracing is recorded from a five-chamber view. Make sure that the orientation of the LVOT is parallel to the Doppler line. You may have to obtain a five-chamber view from a more lateral position. The sample volume should be placed right below the aortic valve. This is accomplished by slowly moving the sample volume back and forth (away and towards the aortic valve). The point at which there is a small but abrupt drop in maximal velocity is the perfect position. The tracing will show a systolic signal below the zero line (flow away from the transducer). The LVOT velocity is used to calculate systolic flow, for example to quantify the area of the aortic valve (continuity equation) or calculate left ventricular stroke volume.
2.5.4 CW Doppler of Aortic Flow Velocity
CW wave Doppler is used to record aortic valve velocity. The signal is recorded from a five-chamber view. Again, make sure you are parallel to transaortic flow. Like the LVOT spectrum, the aortic valve signal will also be "negative". Typically the signal will not start at the onset of the QRS complex, but a little later (after isovolumetric contraction).
Transaortic flow velocity has to be quantified when assessing a stenosis of the aorta or LVOT obstruction (note: the Doppler line also passes through the LVOT). The signal of dynamic LVOT obstruction is "dagger-shaped". More on this aspect is given in Chapter 6, Hypertrophic Cardiomyopathy).
In cases of aortic stenosis it is also necessary to record an aortic valve signal from positions other than the five-chamber view (right parasternal and suprasternal window). Aortic/LVOT velocity can also be recorded from an apical three-chamber view.2.5.5 PW and CW Doppler of the Tricuspid Valve
Spectral Doppler allows us to study both RV inflow and tricuspid regurgitation velocities. RV inflow assessment is performed with PW Doppler from a four-chamber view. Similar to the mitral valve, the sample volume is positioned exactly at the tip of the leaflets. You will also see an M-shaped spectrum with an early and a late filling component. However, compared to the mitral inflow signal, velocities are lower and you will find greater respiratory variations in tricuspid inflow velocities (increase during inspiration).
The uses of RV inflow Doppler are limited. However, it is important for the evaluation of patients with restrictive cardiomyopathy, constrictive pericarditis, and to assess tricuspid stenosis.
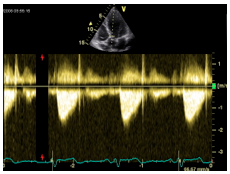
As the tricuspid valve is larger than the mitral valve, the inflow velocities are lower.The signal of tricuspid regurgitation is recorded with CW Doppler. To obtain an adequate signal use an RV-optimized four-chamber view and color Doppler. Sometimes it is necessary to move up one intercostal space. In any case, first optimize your 2D image. The tricuspid valve should be clearly visible. Color Doppler is extremely important since it enables us to document the presence of TR as well as display the direction and origin of the jet. Position the Doppler line through the vena contracta and parallel to the jet. The focus point of the CW Doppler should be at the origin of the jet.
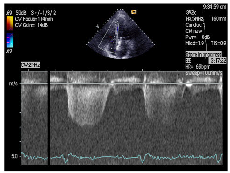
The spectrum of the TR jet will be directed downwards on the tracing. The curve usually has a rounded shape and starts shortly after the onset of the QRS complex.
Optimize the Color Doppler image so that you visualize the vena contracta of the jet. In the presence of eccentric TR jets it may be helpful to use rotational variations of the four-chamber view (such as a two-chamber view of the right heart) to align the CW Doppler to the TR signal.2.5.6 PW Doppler of Pulmonary Venous Flow
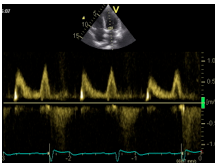
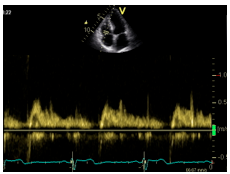
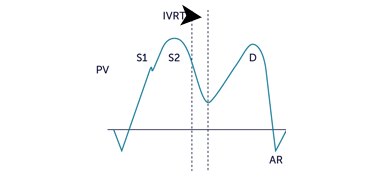
Assessment of pulmonary venous flow is important for evaluation of diastolic function. Regrettably, adequate signals can only be recorded in about 50-60% of patients. Flow is recorded from a four-chamber view from the right upper pulmonary vein. It is recommended to first use color Doppler to visualize flow. Since the flow velocity is rather low, it may be helpful to reduce the Nyquist limit of color Doppler. Place the PW Doppler sample volume at the origin of the vein and reduce the low pass filter of PW Doppler. The pulmonary venous flow curve will consist of a systolic (S1, S2) and a diastolic component (D), with a late diastolic negative deflection (AR). The negative deflection corresponds to atrial contraction and denotes a brief episode of "flow reversal".
2.5.7 Pulsed Wave Doppler of Hepatic Venous Flow
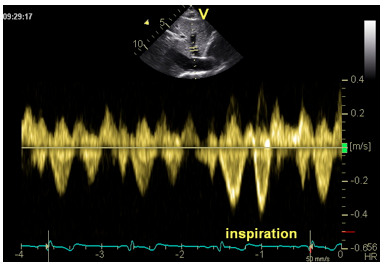
To record systemic venous flow you should use a subcostal view and place the sample volume within a hepatic vein. The orientation of the hepatic veins is more favorable than that of the inferior vena cava (parallel to the insonation angle). It may be difficult to obtain a good spectrum, especially because respiration may easily move the sample volume outside the lumen of the hepatic vein. Record the tracing under "shallow" breathing conditions. However, do not ask the patient to hold his/her breath, because it is important to observe respiratory variations in hepatic venous flow.
The normal spectrum will show a rather low velocity (0.5 - 0.8 m/sec) while the curve will show a systolic and a diastolic flow component. Forward flow (signal below the zero line) increases during inspiration.
Hepatic venous flow is used under restricted or constricted physiological conditions and to detect prominent flow reversal in the presence of severe tricuspid regurgitation.
2.5.8 Other Uses of Spectral Doppler
You can display flow everywhere in the heart. Spectral Doppler has several uses aside from those mentioned above. It can display shunt flow of a ventricular (VSD) or an atrial septal defect (ASD). To find the jet, use color Doppler and find an orientation in which you are parallel to the jet. Use CW Doppler for a VSD and PW Doppler for an ASD. Spectral Doppler is also useful to analyze the nature of jets. Especially in complex pathologies, such as highly eccentric regurgitation and coronary or intracavitary fistulas. Spectral Doppler will help you to determine the phase of the cardiac cycle in which the jet occurs, as well as its direction and velocity.