14. Subclavian Steal Syndrom

14.1 What is the subclavian steal syndrome?
The subclavian steal syndrome is a condition where hypoperfusion of the cerebrovascular system is caused by occlusion (or severe obstruction) of the proximal subclavian or brachocephalic artery. It is characterized by flow reverse in the vertebral artery to supply the vascular bed distal to the occlusion/obstruction and to perfuse the arm (collateral flow). Its prevalence is approximately 2.5%.
14.2 What are some important facts about the subclavian steal syndrome?
The following table lists important facts related to the pathophysiology, findings, symptoms and treatment options in subclavian steal syndrome.
Subclavian steal syndrome - Facts
- Critical stenosis or occlusion of the subclavian artery proximal to the vertebral artery.
- More common on the left side (4:1 ratio left to right), more common in males, relatively benign condition.
- Results in retrograde blood flow in the ipsilateral vertebral artery (collateral flow).
- Leads to blood pressure difference left / right arm.
- Etiology: Atherosclerosis (most common), vasculitis, thoracic outlet syndrome, stenosis of surgical repair (coarctation, Blalock Taussig shunt for Tetralogy of Fallot).
- Often asymptomatic but can cause symptoms of: Vertigo, pre-syncope, syncope, sensorineural hearing loss posterior circulation ischemia) exertional arm weakness.
- Neurological symptoms often occur with exercise of the arm (this “steals blood” from the brain).
- Treatment: Often not needed. Options: surgical (i.e. carotid subclavian bypass) or interventional (balloon angioplasty or stenting). Interventional methods are usually preferred.
- NOTE: Subclavian artery stenosis can also cause „coronary“ subclavian steal syndrome (CSSS) following coronary artery bypass surgery (CABG) with a LIMA (left internal mammary graft) - here you will find retrograde LIMA flow and coronary ischemia.
14.3 How can you quantify the subclavian steal syndrome?
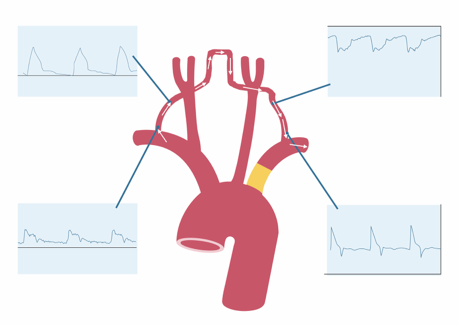
The degree of the subclavian steal syndrome is classified based on the degree of stenosis and the magnitude / consistency retrograde flow in the vertebral artery
Grading of Subclavian Steal syndrome
Stage I: Mild subclavian stenosis < 70%
Findings: Antegrade flow (flow reversal) during provocation maneuver of the arm possible, increased systolic deceleration

Stage II: Moderate so severe subclavian stenosis (> 70%)
Findings: Systolic transient retrograde flow + antegrade diastolic flow (back and forth flow)

Stage III: Occlusion / subtotal occlusion (95-100%)
Findings: Complete flow reversal

14.4 How to assess the subclavian steal syndrome with carotid ultrasound
- Be aware of the typical symptoms of the subclavian steal syndrom. This will raise your suspicion!
- It is important to check direction of flow of the VA (Color Doppler + spectral Doppler) in every patient.
- The absence of flow reversal does not fully exclude a subcalvian steal syndrome. Patients in stage I and II might have incomplete flow reversal. Therefore you should also look at the shape of the spectrum.
- Perform provocation maneuvers: Inflate blood pressure cuff > 20 mmHg above systolic blood pressure for a few minutes. Deflate cuff (causes rapid increase of blood flow in the arm). This will damask the subclavian steal by causing flow reversal in the ipsilateral vertebral artery
- Measure blood pressure on both arms and look for a difference >20-40 mmHg. The degree of difference is correlated with severity of SC stenosis / symptoms.
- Don’t forget to also image the subclavian artery to directly detect the stenosis.
- If you have the suspicion use MRI and CT-Angio to confirm your findings.


14.5 What is the mammary steal syndrom?
The mammary steal syndrom can occur in patients following left internal mammary bypass surgery in the presence of a subclavian artery stenosis. In this circumstance collateral (retrograde) form the mammary bypass graft to the distal subclavian artery can led to ischemia and symptoms of angina. Therefore it is important to detect and exclude a subclavian artery stenosis in patients scheduled for mammary coronary artery bypass graft.

If you like the way we teach, please leave a message!