
Identical Hearts?





Have you ever wondered whether identical twins look the same on the outside as well as the inside? How similar do their hearts look?

When Hans came to the lab to check for the cause of dyspnea and told us that he has an identical twin we knew this was our chance.
 Hans and Paul in 1945
Hans and Paul in 1945
Needless to say, we didn’t find a cause for Hans’s dyspnea in the echo study. But his heart definitely is not normal. What do you think?
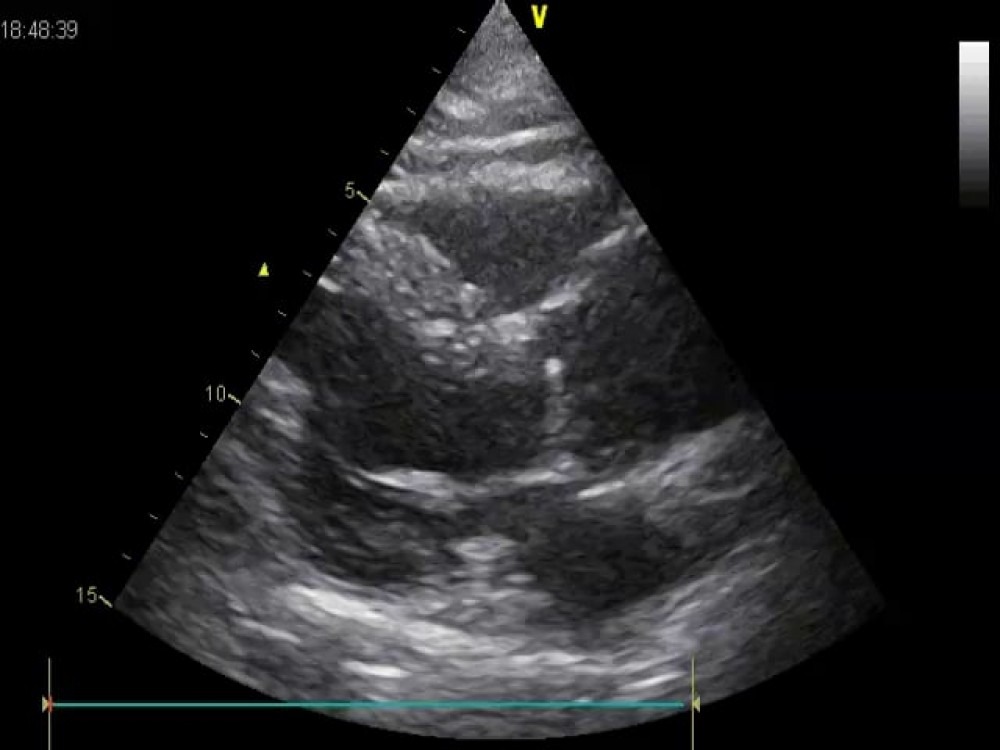 The ascending aorta is dilated. Normal values for the ascending aorta are
22-36mm or 15 mm/m². The size is strongly related to body surface area and age!
The ascending aorta is dilated. Normal values for the ascending aorta are
22-36mm or 15 mm/m². The size is strongly related to body surface area and age!
The ascending aorta is dilated. Normal values for the ascending aorta are 22-36mm or 15 mm/m². The size is strongly related to body surface area and age!
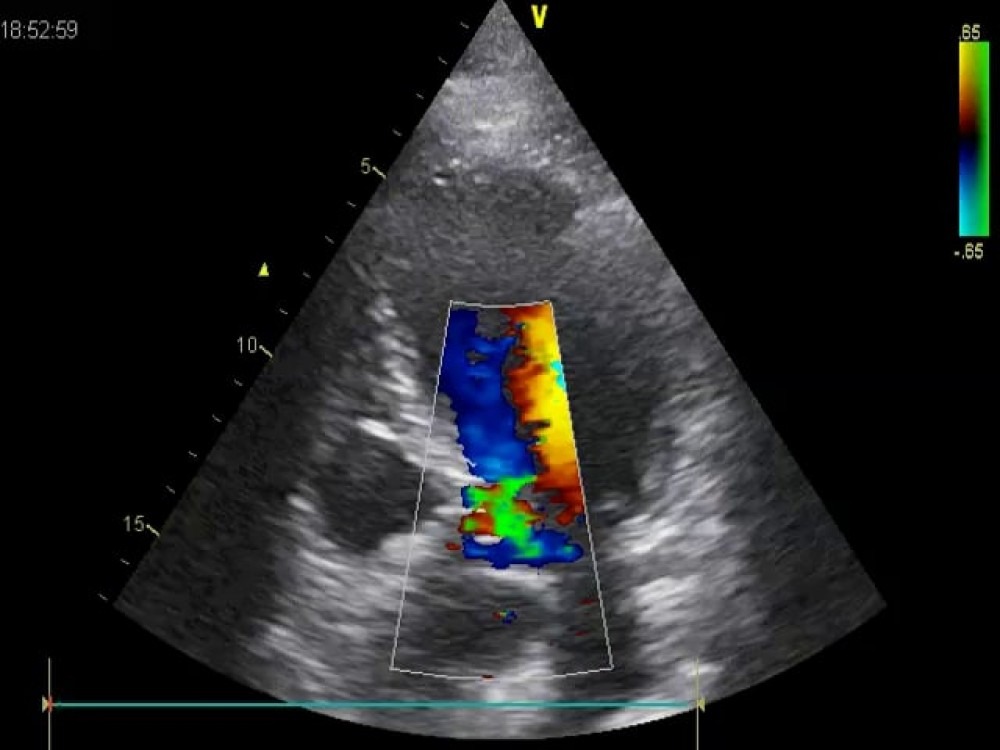 The apical five chamber view shows mild aortic regurgitation.
The apical five chamber view shows mild aortic regurgitation.
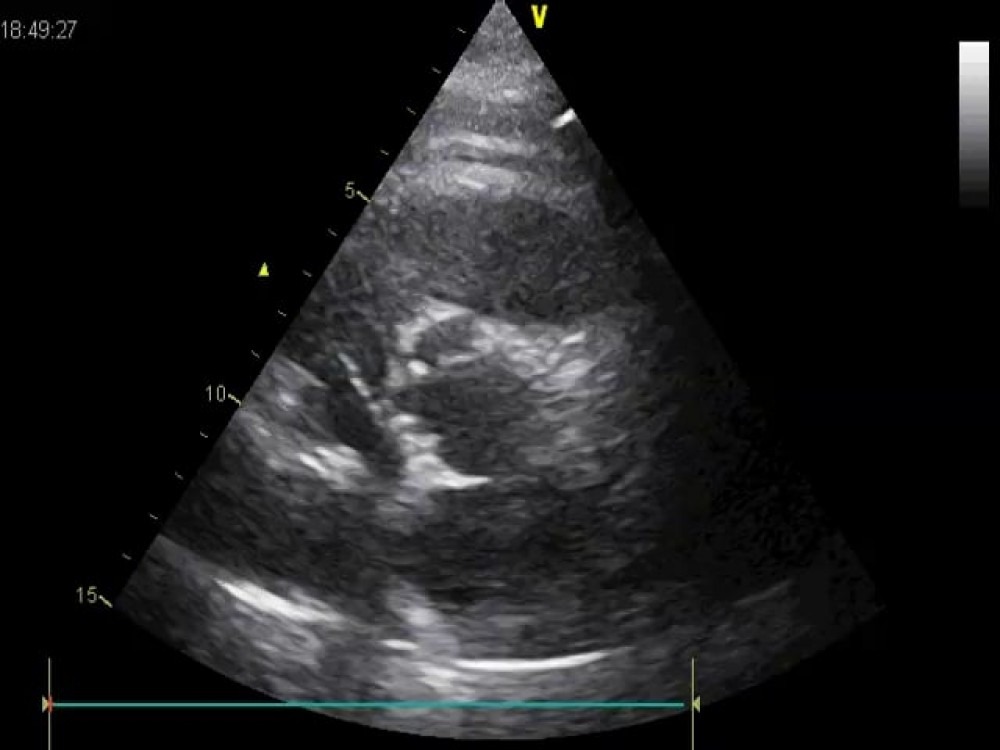 The image quality is not perfect. Can you still see three cusps?
The image quality is not perfect. Can you still see three cusps?
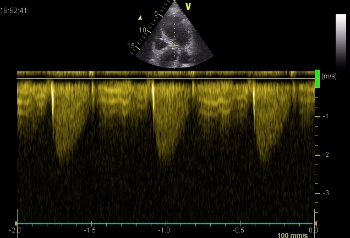 Maximum AV velocity is elevated: 2.2 m/s.
Maximum AV velocity is elevated: 2.2 m/s.
There are several causes of a dilated aorta. Arterial hypertension is certainly the most common, but also connective tissue disease and, last but not least, patients with bicuspid aortic valves frequently present with a wide ascending aorta.
Why is Hans’s aorta dilated? Is his aortic valve bicuspid? Very difficult to say from the images. Remember: patients may have a very subtle raphe and might appear tricuspid, but functionally they are bicuspid.
What about the twin brother?
We called his brother in. Truly they were identical twins, hard to distinguish. We put the transducer on the chest and - wow -Paul’s heart mirrored that of his brother. Have a look yourself:
Hans - Paul


Identical hearts?
Mild and also a dilated aorta. Was this another hint that their valves were congenitally abnormal? Should we perform a TEE? Paul has coronary artery disease and had already received two stents. Should we also perform a coronary angiogram on his brother?
Heart disease in twins
Twin studies draw a lot of attention because they can help to sort out what is inherited and what is environmental - especially when the twins were separated early and live independent lives. In 20,000 Swedish twins that were followed over 36 years, genetic factors seemed to play a more important role in predicting death from coronary heart disease (CHD) in early vs. later life (Zdravkovic S et al., 2002). CAD is a complex disease with many risk factors contributing to morbidity and mortality. Risk factors like hyperlipidemia, arterial hypertension, and diabetes mellitus are influenced by genetic factors and lifestyle. Obviously, both factors are much more similar in twins than in two random individuals of the general population (Austin et al., 1987, Evans A et al., 2003).
Our twins had a rather healthy lifestyle and had not suffered from any severe disease in the first six decades of their lives. They are a little overweight and had mild arterial hypertension for a few years. Our patients presented with a dilated aorta and mild aortic stenosis at a rather young age. Both could be explained well by a bicuspid aortic valve.
Why should we care?
With a prevalence of 1-2% in the general population, bicuspid aortic valves are the most common congenital valve pathology. Over the years, progressive calcification of the bicuspid valve may lead to significant stenosis and/or significant aortic regurgitation and aneurysm of the ascending aorta. But what does it mean when a family member or even my twin brother or sister is diagnosed with a bicuspid valve?
Bicuspid valves in identical twins
A few case reports have been published, describing bicuspid aortic valves in identical twins (Saravanan P et Kadir I, 2009; Brown C et al., 2003). Other studies looked at relatives of patients with bicuspid valves. In these screenings, up to 31% of the relatives also had bicuspid aortic valves or other cardiovascular malformations such as aortic dilatation, coarctation, VSD or ASD, abnormal mitral valves, or a hypoplastic left heart syndrome (Cripe L et al., 2004). Another study found bicuspid valves in 9% of screened first-degree relatives of patients with known bicuspid valves. In the same study, 12% of the screened relatives had a dilated ascending aorta (Huntington K et al., 1997).
What is the take-home message? If you have a twin sibling with a heart problem, it is probably wise to get an echo and further testing done as well.
 Hans and Paul in August 2014
Hans and Paul in August 2014
More identical hearts?
What are your thoughts? Do you have any identical-heart-stories to tell?
Share your experiences and leave a comment.
PS: many thanks to Hans and Paul for providing their photos!
1. Austin MA et al. Risk factors for coronary heart disease in adult female twins. Genetic heritability and shared environmental influences. Am J Epidemiol. 1987 Feb;125(2):308-18.
2. Brown C, Sane DC, Kitzman DW. Bicuspid aortic valves in monozygotic twins. Echocardiography. 2003 Feb;20(2):183-4.
3. Cripe L, Andelfinger G, Martin LJ, Shooner K, Benson DW. Bicuspid aortic valve is heritable. J Am Coll Cardiol. 2004 Jul 7;44(1):138-43.
4. Evans A et al. The genetics of coronary heart disease: the contribution of twin studies. Twin Res. 2003 Oct;6(5):432-41.
5. Huntington K, Hunter AG, Chan KL. A prospective study to assess the frequency of familial clustering of congenital bicuspid aortic valve. J Am Coll Cardiol. 1997 Dec;30(7):1809-12.
6. Saravanan P, Kadir I. Apolipoprotein E alleles and bicuspid aortic valve stenosis in monozygotic twins. Interact Cardiovasc Thorac Surg. 2009 Jun;8(6):687-8. doi: 10.1510/icvts.2009.203273. Epub 2009 Mar 20.
7. Zdravkovic S et al. Heritability of death from coronary heart disease: a 36-year follow-up of 20 966 Swedish twins. Journal of Internal Medicine 2002;252: 247–254
Related Courses

The Echo BachelorClass provides an invaluable foundation for the practice of echocardiography…